PATHOLOGIES
Ullrich dystrophyULLRICH DYSTROHPHY
WHAT IS
Ullrich congenital muscular dystrophy is a genetic disorder involving certain genes encoding for the alpha chains of Collagen VI (COL6A1, COL6A2 and COL6A3), most of the known cases being autosomal recessive inherited.
This congenital muscular dystrophy is characterised by a slow but early progression, relatively generalised weakness, hyperlaxity of the distal joints (hands, fingers, toes, etc.) and contractures on the proximal ones (elbows, ischiocratic quadriceps, etc.). At birth, particular signs can be observed, such as transient kyphosis, contractures at the elbows and knees, a cleft palate, torticollis, weakness of the somatic muscles and distal hyperlaxity. The skin may also show typical signs such as follicular hyperkeratosis, keloid formation in wound healing and thick, velvety skin. Individuals with this congenital dystrophy are often confined to a wheelchair as they walk independently for only a short time. Respiratory difficulties can be observed in the most severe cases.
CLINICAL ASPECT of ULLRICH DMC
1- weakness of muscles and hypotonia present at birth;
2- coexistence of retractions and distal hyperlaxity;
3- walking not acquired or lost in the first decade
4- early respiratory insufficiency and scoliosis.
IN COMMON WITH OTHER PATHOLOGIES:
– preserved intelligence;
– presence of skin changes: keloids, exuberant or thin scars, wrinkled skin = (follicular hyperkeratosis);
– CPK (serum creatine phosphokinase) value normal or variably elevated;
– no cardiac involvement;
– respiratory muscle impairment: constant and early in Ullrich CMD – variable and late in Bethlem myopathy.

Prominent heel
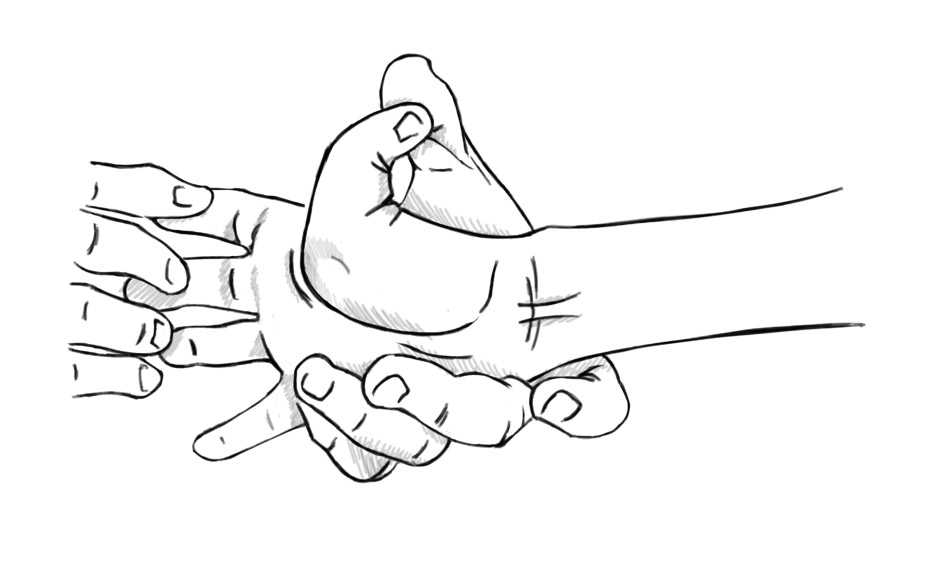
Joint hypermobility
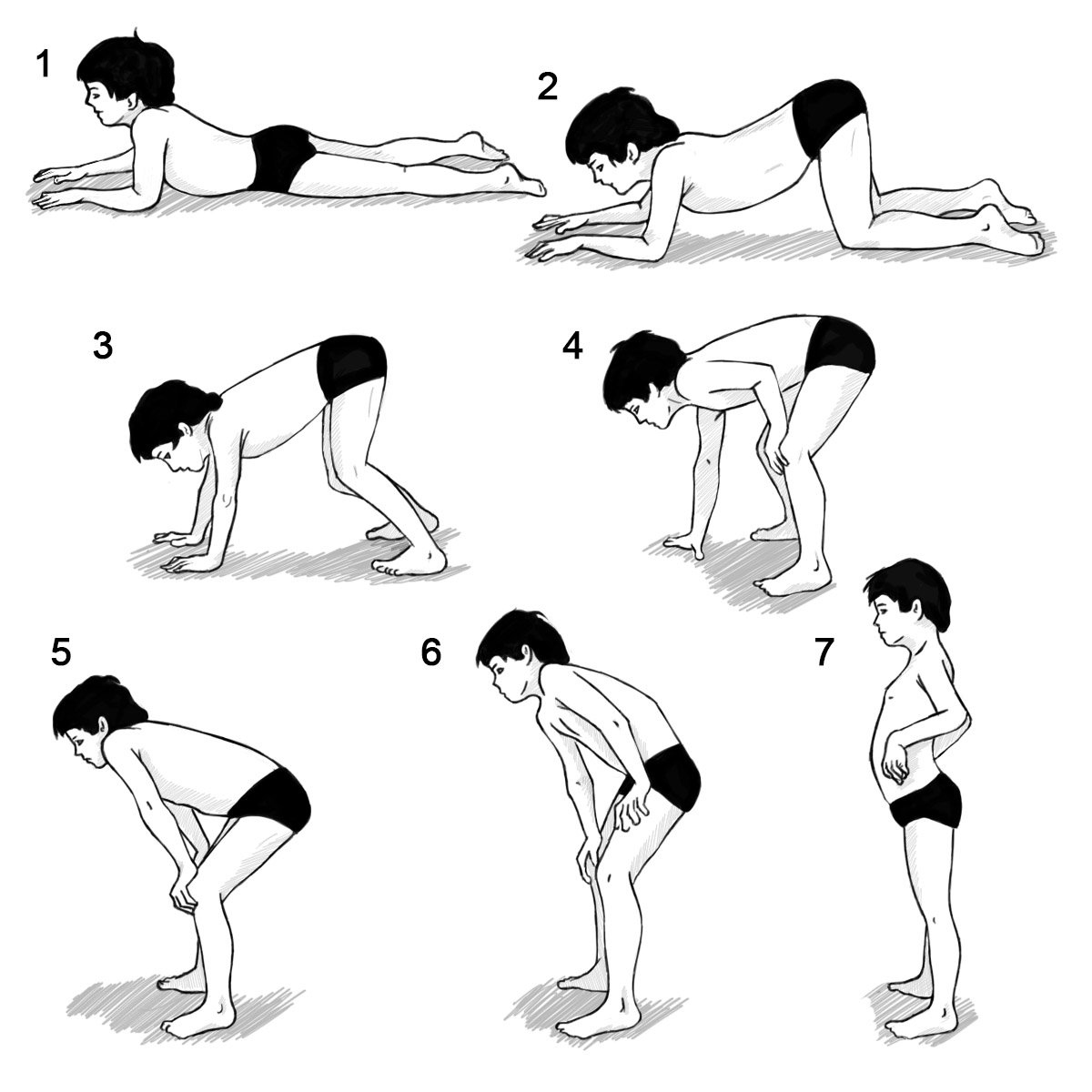
Gowers’ Sign

Retractions in the Achilles tendons
Inheritance
Ullrich CMD is inherited in an autosomal dominant (one mutation is sufficient to cause the disease) or recessive (two mutations are required) manner; the myosclerotic variant is inherited in a recessive manner only. If the inheritance is dominant, it may happen that one of the parents is affected (the one who transmitted the mutation) or both are unaffected if the mutation arose de novo.
If the inheritance is recessive, the parents of the affected person are usually healthy carriers. The offspring of the affected person are healthy carriers.
Once the mutation has been identified, it is possible to assess the risk of transmission of the disease and propose a prenatal diagnosis in high-risk pregnancies.
Prophylaxis of respiratory infections
Vaccination, physiotherapy and early administration of antibiotics.
Checks and treatment for Ullrich CMD
- periodic check of muscle strength, functional capacity (standing, walking, stairs), joint motility (retractions and hyperlaxity).
- growth and nutritional status; there may be difficulty in feeding due to muscular and respiratory fatigability, percutaneous endoscopic gastrostomy may be necessary.
- respiratory assessment, ease of infection immediate broncho-pulmonary treatment, spirometry, nocturnal oximetry, respiratory physiotherapy, cough machine, mechanical ventilation.
- spine inspection for scoliosis, X-ray under load, orthopaedic check for dislocation also possible surgical indications for correction of retractions or scoliosis.